





Miller’s Pyramid in Medical Education: A Practical Guide to Competency-Based Assessment
Competency-based education is no longer just a trend—it is the foundation of modern medical education. While knowledge remains essential, healthcare professionals must also demonstrate clinical skills, sound judgment, and professional behavior in real-life situations.
One of the most widely used frameworks for assessing competence is Miller’s Pyramid, developed by Dr. George E. Miller in 1990. Despite being over three decades old, it continues to guide curriculum design, teaching, and assessment in medical schools worldwide.
Let’s understand it in a practical way.
What Is Miller’s Pyramid?
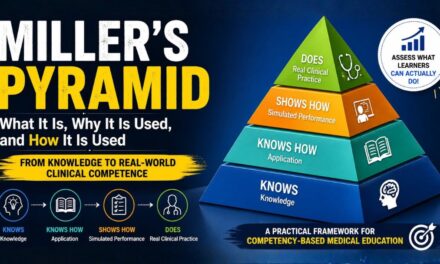
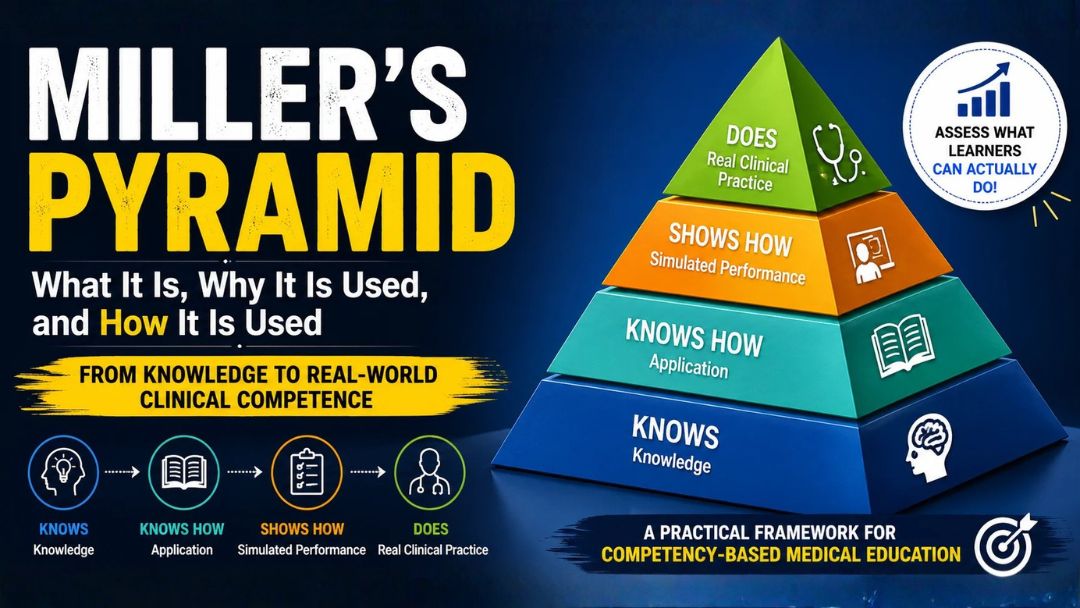
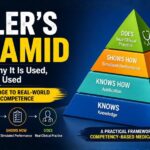
Miller’s Pyramid is a four-level framework that describes how learners progress from acquiring knowledge to performing competently in real clinical practice.
Instead of asking only,
“Does the student know the answer?”
Miller’s Pyramid asks,
“Can the student actually perform safely and effectively with real patients?”
The model moves from knowledge → competence → performance → professional practice.
DOES
Real Clinical Practice
SHOWS HOW
Simulated Performance
KNOWS HOW
Application
KNOWS
KnowledgeWhy Is Miller’s Pyramid Important?
Traditional education often focuses heavily on written examinations.
However, scoring well in theory does not necessarily mean someone can:
- Examine a patient
- Communicate effectively
- Perform a procedure safely
- Make appropriate clinical decisions
Miller’s Pyramid ensures that assessment measures what learners know and what they can actually do.
This makes education more aligned with patient care and real-world clinical practice.
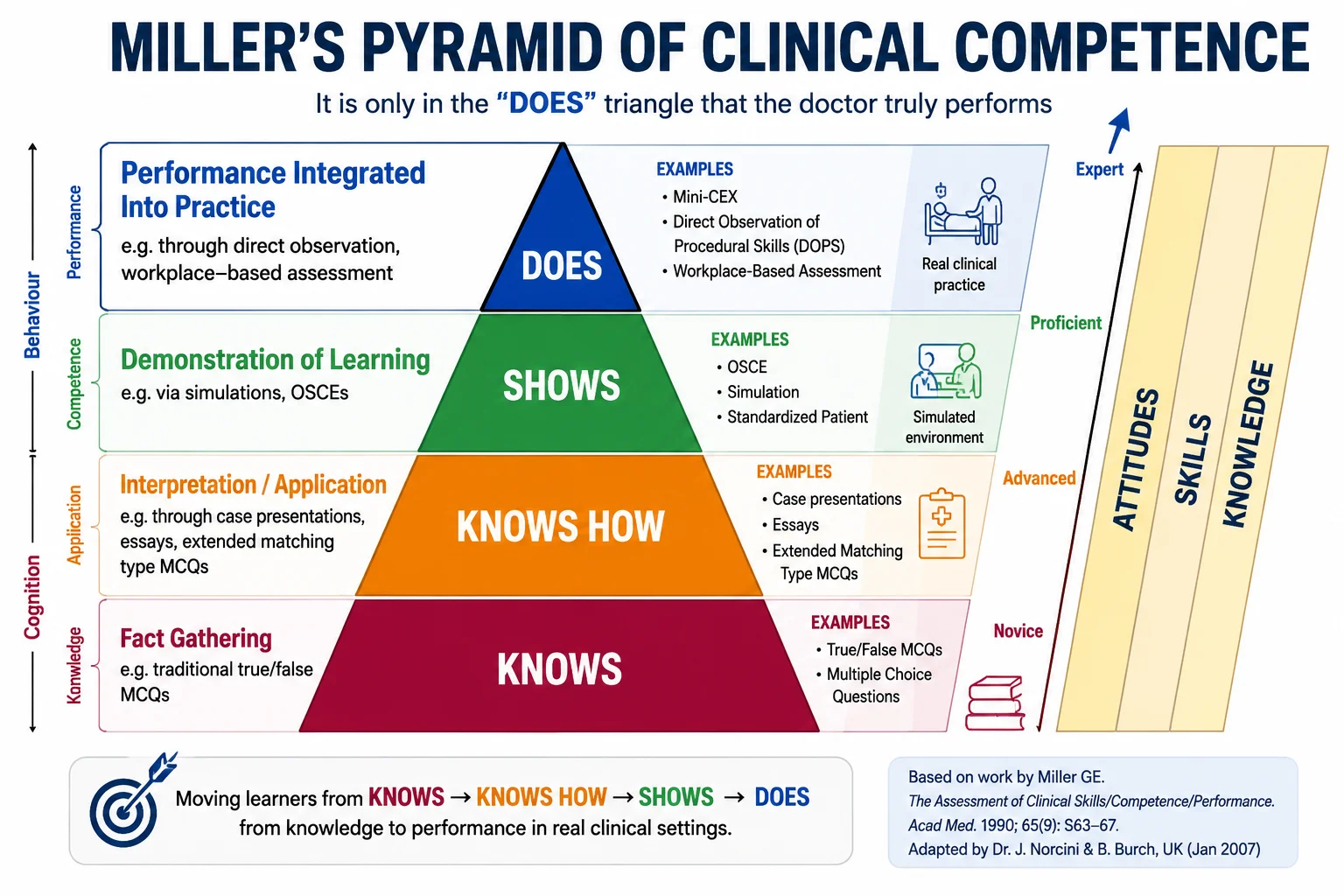
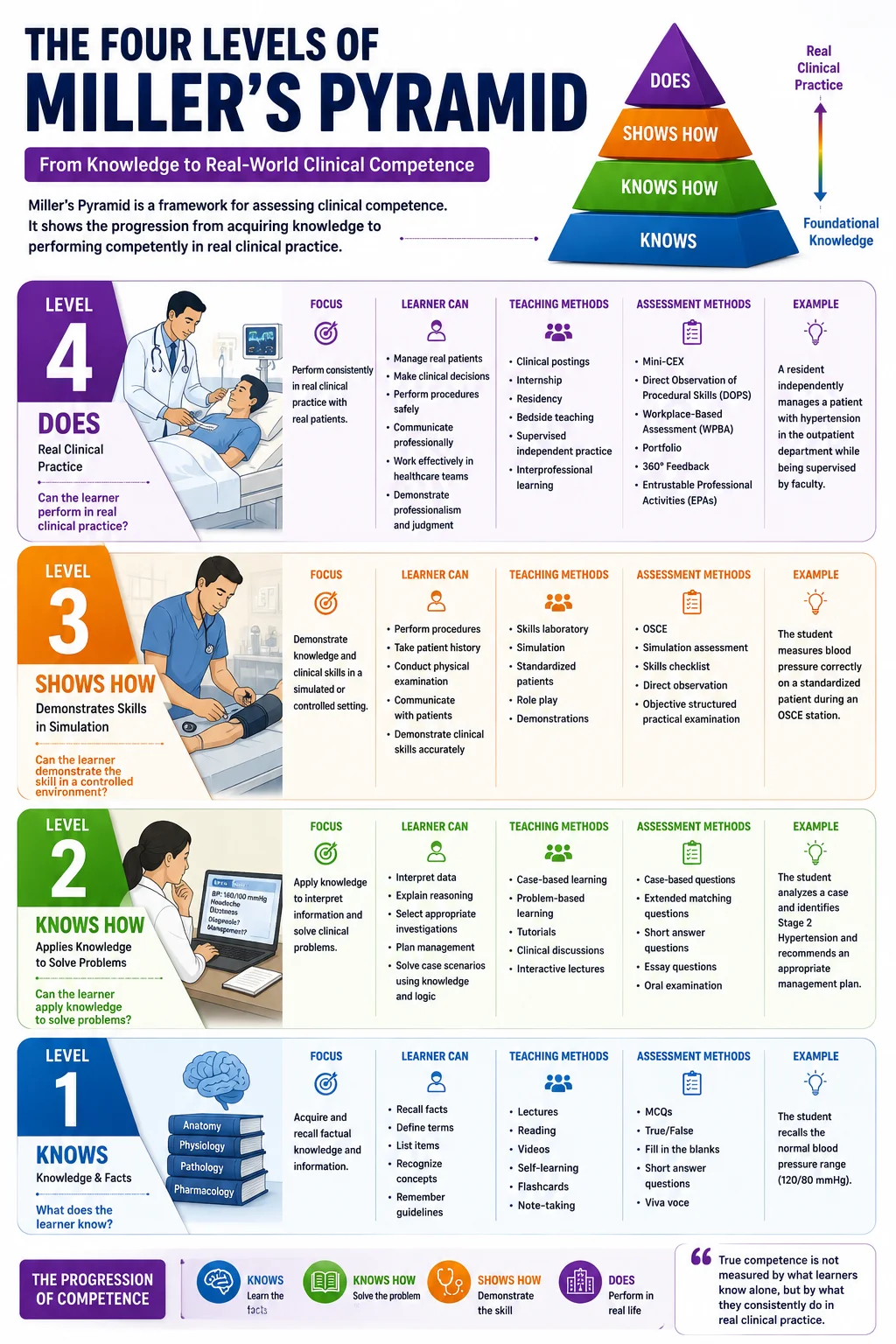
The Four Levels of Miller’s Pyramid
Level 1 — Knows
Question:
What does the learner know?
This is the foundation.
Students acquire factual knowledge, concepts, definitions, and principles.
Examples
- Anatomy
- Physiology
- Pharmacology
- Clinical guidelines
Typical Assessments
- Multiple Choice Questions (MCQs)
- Short Answer Questions
- Viva
- Written examinations
Example
A student correctly explains the causes of hypertension.
The student possesses knowledge.
Level 2 — Knows How
Question:
Can the learner apply the knowledge?
At this stage, learners begin solving problems rather than simply recalling facts.
Examples
- Clinical reasoning
- Case discussions
- Diagnosis
- Treatment planning
Typical Assessments
- Case-based questions
- Problem-Based Learning (PBL)
- Extended Matching Questions
- Clinical scenarios
Example
A student reviews a patient’s symptoms and identifies the likely diagnosis of hypertension with an appropriate management plan.
Knowledge is now being applied.
Level 3 — Shows How
Question:
Can the learner demonstrate the skill?
This is where students perform tasks in a controlled or simulated environment.
Examples
- Physical examination
- History taking
- Suturing
- CPR
- Communication skills
Typical Assessments
- OSCE
- Skills laboratory
- Simulation
- Standardized patients
Example
The student performs blood pressure measurement correctly during an OSCE station.
The learner demonstrates competence under observation.
Level 4 — Does
Question:
Can the learner perform consistently in real clinical practice?
This is the highest level of the pyramid.
Assessment focuses on actual workplace performance rather than simulation.
Examples
- Managing real patients
- Clinical decision making
- Teamwork
- Professionalism
- Patient communication
Typical Assessments
- Mini-CEX
- Direct Observation of Procedural Skills (DOPS)
- Workplace-Based Assessment (WPBA)
- Entrustable Professional Activities (EPAs)
- Portfolio assessment
- 360-degree feedback
Example
A resident independently manages patients with hypertension in the outpatient department while being supervised by faculty.
This reflects real competence.
A Practical Example
Imagine teaching blood pressure measurement.
| Miller Level | Learning Activity | Assessment |
|---|---|---|
| Knows | Learn normal BP values and hypertension guidelines | MCQ |
| Knows How | Interpret a patient’s BP readings | Case discussion |
| Shows How | Measure BP on a simulated patient | OSCE |
| Does | Measure BP accurately during clinical postings | Workplace observation |
Notice how the assessment becomes progressively more authentic.
How Educators Use Miller’s Pyramid
Miller’s Pyramid helps faculty align teaching with assessment.
A simple workflow is:
- Define the competency.
- Write measurable learning objectives.
- Choose appropriate teaching methods.
- Select assessments that match the learner’s stage.
- Provide feedback and opportunities for improvement.
For example:
Competency
“Perform a cardiovascular examination.”
| Stage | Teaching | Assessment |
|---|---|---|
| Knows | Lecture | MCQ |
| Knows How | Clinical case discussion | SAQ |
| Shows How | Skills lab | OSCE |
| Does | Clinical posting | Mini-CEX |
This alignment ensures learners are assessed fairly and meaningfully.
Strengths of Miller’s Pyramid
- Simple and easy to understand.
- Links knowledge with real-world performance.
- Supports competency-based medical education (CBME).
- Encourages authentic assessment.
- Widely accepted in medicine, nursing, dentistry, and allied health education.
- Helps educators select the right assessment for the right learning outcome.
Limitations
Although highly valuable, Miller’s Pyramid has some limitations.
- Clinical performance may vary depending on the workplace.
- Real-world assessment requires trained faculty and observation.
- Professional attitudes and lifelong learning are difficult to measure using the pyramid alone.
- Modern competency frameworks often combine Miller’s Pyramid with EPAs and workplace-based assessments.
Key Takeaways
Miller’s Pyramid reminds educators that knowledge alone is not competence.
A learner progresses through four stages:
- Knows – understands the facts.
- Knows How – applies knowledge to solve problems.
- Shows How – demonstrates skills in a simulated setting.
- Does – performs competently in real clinical practice.
The most effective educational programs assess learners at all four levels, ensuring graduates are not only knowledgeable but also capable of delivering safe, effective, and patient-centered care.
Final Thought
In competency-based education, the ultimate goal is not simply to produce students who can pass examinations—it is to develop healthcare professionals who can apply knowledge, demonstrate skills, and consistently deliver high-quality patient care. Miller’s Pyramid provides a clear roadmap for achieving this by ensuring that assessment progresses from knowing to doing, making learning more meaningful, authentic, and aligned with real clinical practice.
This post may contain affiliate links, which means I may earn a commission for purchases made through these links. Your support will encourage us to continue adding value to you through blogs like this. Learn more on my Private Policy page.




{kind=link}